
How do we Hear?
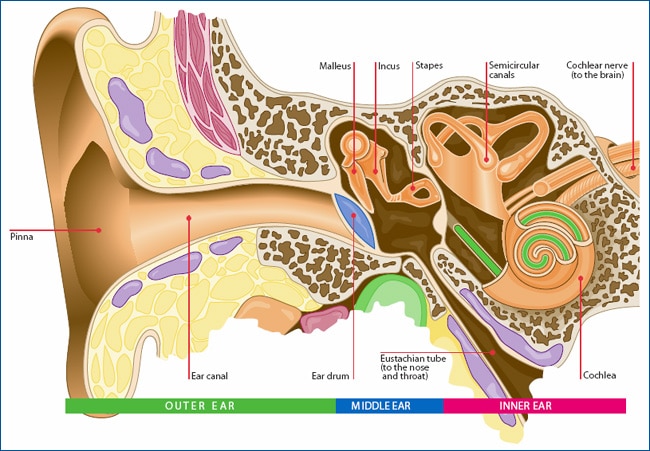
There are 3 main parts of our hearing system; the outer ear, middle ear and inner ear.
Outer Ear:
Our outer ear is the part we see. It is made up of the pinna and the ear canal that directs the sounds we hear down to our middle ear. The shape of the pinna plays an important role in helping us locate where sounds are coming from, and to focus and attend to the person talking in front of us.
The outer part of our ear canal is lined with tiny hairs that assist in making wax. Wax is important to protect our ear from anything entering it. Cotton buds are not recommended to clean our ears as they damage these delicate hairs and our ears’ natural cleaning process. Wax is only a problem if it completely blocks the ear canal.
Middle Ear:
Our middle ear includes the eardrum (tympanic membrane) and the ossicles (the 3 smallest bones in the body, the malleus, incus, and stapes). Sound enters our ear canal from our outer ear, vibrates our eardrum which in turn vibrates our ossicles. High pitch sounds cause fast vibrations and low pitch sounds cause slow vibrations.
The ossicles are in the perfect position to increase the energy of sounds we hear, prior to them entering our inner ear. Our inner ear is filled with fluid and without this increase in energy, sound vibrations would be significantly reduced going from air to fluid (e.g., we need to more energy walking through water at the beach (fluid) than walking on the sand (air)).
Inner Ear:
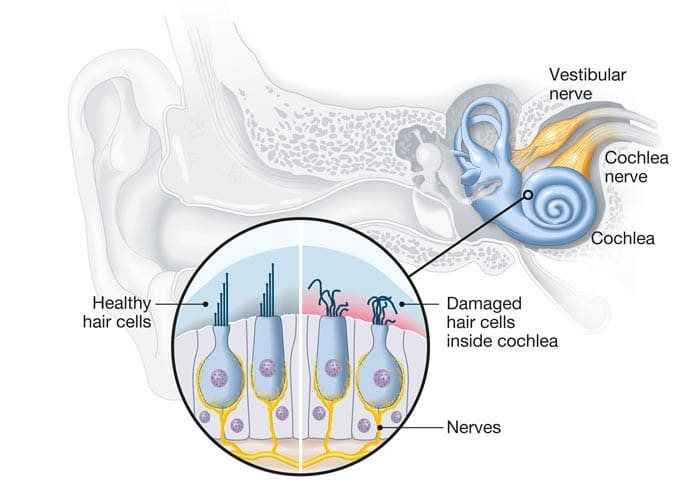
Our inner ear is made up of the cochlea and semi-circular canals. The cochlea is about the size of a pea and shaped like a small shell. It is responsible for converting sound vibrations from the middle ear into electrical impulses (neural signals) that are sent along the auditory nerve to our brain. Inside our cochlea are approximately 15,000 delicate hair cells (3,500 inner hair cells and 12,000 outer hair cells). The inner hair cells do most of the work sending signals to our brain, however the outer hair cells are important to help the inner hair cells to process soft sounds.
When sound vibrations enter our cochlea, a wave of fluid moves over our inner ear hair cells, bending them back and forth and triggering an electrical (neural) impulse. The hair cells are positioned precisely to represent different pitches. The fluid wave has the most energy at the pitch we need to hear. The neural impulse travels up our auditory nerve to our brain (auditory cortex). When sounds reach our brain, our past experiences, knowledge, and memory make sense of what we have heard.
Our semi-circular canals are made up of three tiny, fluid filled tubes, each positioned at a different angle to help us balance. When we move our head, the fluid inside these hair cell lined tubes also moves, bending the hair cells back and forth. This causes a neural impulse to be sent to our brain with information about our position and what we need to do to stay balanced. If we spin around and then suddenly stop, we feel dizzy as it takes the moving fluid a little longer to stop.
What are the Types and Causes of Hearing Loss?
 It is estimated that 1 in 6 Australians have some degree of hearing loss. Further, research suggests that approximately 1 in 1000 children have hearing loss at birth. A further 1 in 1000 are not detected until school age, i.e., the number of children with hearing loss doubles by school age (Hearing Australia, 2014). For infants diagnosed at birth, approximately 50% have no risk factors for hearing loss and the cause remains unknown.
Undetected hearing loss can have a significant effect on a child’s development (i.e., their speech& language, social skills, behaviour, and academic progress). Detecting hearing loss early is important to make sure your child is supported and has every opportunity to reach their full potential.
Damage to any of the three parts of our ear can cause hearing loss.
Hearing loss is described using:
It is estimated that 1 in 6 Australians have some degree of hearing loss. Further, research suggests that approximately 1 in 1000 children have hearing loss at birth. A further 1 in 1000 are not detected until school age, i.e., the number of children with hearing loss doubles by school age (Hearing Australia, 2014). For infants diagnosed at birth, approximately 50% have no risk factors for hearing loss and the cause remains unknown.
Undetected hearing loss can have a significant effect on a child’s development (i.e., their speech& language, social skills, behaviour, and academic progress). Detecting hearing loss early is important to make sure your child is supported and has every opportunity to reach their full potential.
Damage to any of the three parts of our ear can cause hearing loss.
Hearing loss is described using:
- where the issue occurs (i.e., outer, middle, or inner ear)
- whether one or both ears are affected (unilateral or bilateral)
- when the loss occurred – i.e., present at birth (congenital), progressive, or acquired (e.g., illness, medication, injury).
- degree (level) of hearing loss (mild, moderate, severe, or profound)
Sensorineural Hearing Loss (SNHL)
Occurs in the inner ear and is permanent in nature. Causes may include:- Complications at birth, (including prematurity, low birth weight)
- Family history of hearing loss / genetics (most common Connexin 26)
- Frequent middle ear infections
- Infections such as meningitis or cytomegalovirus (CMV)
- Syndromes (e.g., CHARGE)
- Chronic noise exposure
- Age-related progressive loss
Conductive Hearing Loss (CHL)
Occurs in the middle ear or ear canal and may be either temporary or permanent depending on the cause. Causes may include:- Ear infections or middle ear fluid (often referred to as glue ear)
- Wax impaction (wax completely blocking the outer ear canal)
- Damage or stiffening of the ossicles (middle ear bones)
- Cyst in the middle ear (cholesteatoma)
- Bony growth along the ear canal (exostoses, often referred to as swimmer’s ears)
Mixed Hearing Loss
Occurs when there is a combination of middle ear and inner ear pathology. These losses typically require both medical and audiological management.What are the Degrees of Hearing loss?
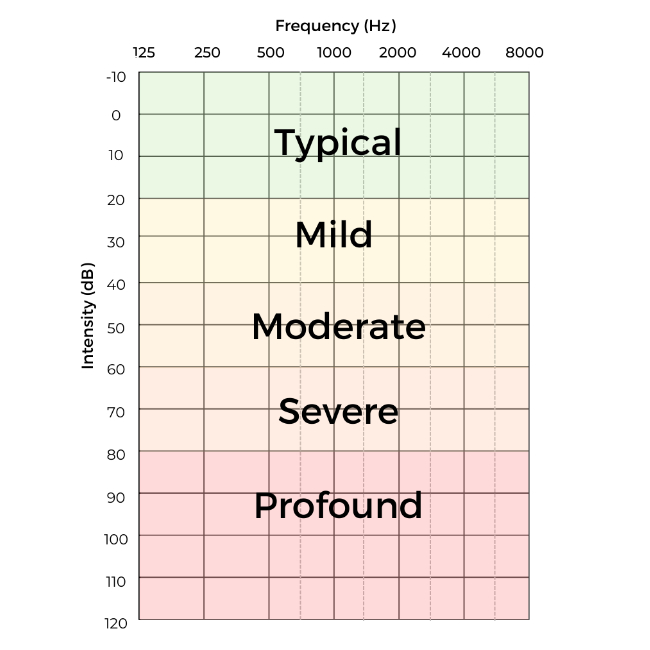 Hearing loss can be described as within normal limits, mild, moderate, severe, or profound. The softest sounds your child can hear are measured and marked on a graph, called an audiogram. From left to right across the graph represents low pitch (125Hz) to high pitch (8000Hz) sounds (frequencies) and from the top of the graph (-10dB) to the bottom of the graph (120dB) represents the softest to loudest sounds.
Hearing loss can be described as within normal limits, mild, moderate, severe, or profound. The softest sounds your child can hear are measured and marked on a graph, called an audiogram. From left to right across the graph represents low pitch (125Hz) to high pitch (8000Hz) sounds (frequencies) and from the top of the graph (-10dB) to the bottom of the graph (120dB) represents the softest to loudest sounds.
Mild Hearing Loss
If your child has a mild hearing loss (between 21dB and 40dB), they may;- miss soft speech or speech at a distance
- often ask others to repeat information
- have difficulty following conversations, particularly in the presence of background noise
- tire quickly – listening is challenging
- benefit from hearing aids or the use of a personal listening device (remote microphone)
Moderate Hearing Loss
If your child has a moderate hearing loss (between 40dB and 60dB), they will;- have increasing difficulty understanding normal level conversations
- be unable to hear some speech sounds
- struggle listening in groups and in noisy environments
- tire quickly – listening is challenging
- need to wear hearing aids to access speech
- likely benefit from the use of a personal listening device (remote microphone)
Severe Hearing Loss
If your child has a severe hearing loss (between 60dB and 80dB), they will;- be unable to hear others speaking at normal conversation levels
- struggle to hear in all listening environments without the use of hearing aids
- tire quickly – listening is challenging
- have difficulty hearing in the presence of background noise, or at a distance, even when using hearing aids
- benefit from the use of a personal listening device (remote microphone) remote microphone
Profound Hearing Loss
If your child has a profound hearing loss (hearing levels > greater than 80dB), they will- not hear others speaking at loud conversation levels
- heavily rely on visual information
- have hearing and listening difficulties, especially in noise, over distance and in groups even when using hearing aids


